To Cement or Not: The Evolution of Partial & Total Knee Replacement
Arthritic knees hurt. Resurfacing them with metal and polyethylene inserts provides pain relief and a return to activities—a godsend for people losing mobility due to arthritis. Traditionally, people with these artificial components in their knees have been advised to relatively “rest” and protect their joints so that they would last a lifetime.

For the last 35 years, we have given the opposite advice—and here is why.
As you age, you naturally lose muscle and bone. The only effective therapy to counter this process is daily resistance exercise, such as weightlifting, hill and stair climbing, and active exercise classes (with bouncing and jumping). Bone and muscle respond to stress with the formation of more bone and muscle.
Telling a patient to rest their joint leads to more bone and muscle loss, and a greater chance of the replacement joint loosening than does doing exercise. Even impact exercise. Even running. Over 35 years of telling patients to go and do as much as they can physically and in sports, we have seen exactly one patient wear out their components, and that was possibly due to sports.
Yet some joints do come loose, and there is a significant failure rate of artificial knee joint replacement. The most common reason is loosening of the cement used to fix many metal joints to the bone (polymethylmethacrylate). This cement was invented in 1958 by Sir John Charnley for hip replacements and spread widely to knee replacement in the 1980s.
Charnley’s cement provided strong fixation and permitted patients to walk on their replaced joints immediately. However, it also led to complications: cement/bone and cement/prosthesis interface loosening.
Cementless designs were created by Peter Walker and John Insall in the 1980s, but they required very precise bone cuts that were not routinely possible for most surgeons using the then-available saw guides and alignment devices.
This changed with the introduction of the MAKO robot in 2006. Martin Roche first used it to perform partial knee replacements, which previously had been difficult to align correctly for each patient. In 2015, the FDA cleared the robot for total (not yet partial) knee replacement, and I bought the first outpatient robot in the US in 2016. While I had considered myself a pretty good joint replacement surgeon beforehand, the robot permitted me to be so much more precise that it opened up the revolutionary possibility of using cementless components for all my total knee replacements.
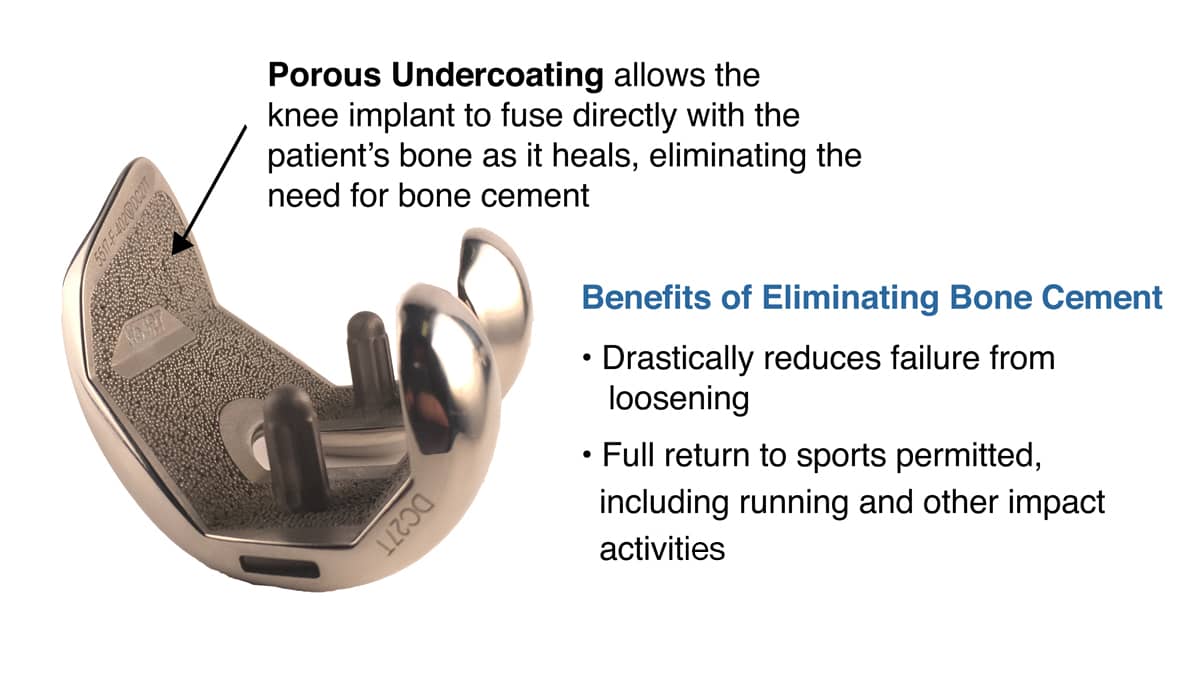
Without cement, my patients need have no fear of returning to running and impact sports on their replaced knees. To knock the components loose, they would essentially have to break their leg. Advances in the polyethylene tray component of the device give them, supposedly, at least 30 years of durability. None have worn out yet.
Unfortunately, the cementless advances don’t yet apply to the partial knee components. Most likely, it is because the surface area of the partial components is so small that the bony fixation is not as strong.
Though this advance is on the horizon, some of my patients aren’t waiting. One of them ran across the US on his bilateral partial knees. I can’t catch him.
An Ultramarathoner Told He Would Never Run Again
Richard Donovan is an ultramarathon runner known for extreme endurance challenges. When knee arthritis threatened his ability to run, he was given the familiar advice: stop running, wait for knee replacement, and accept that the sport he loved was behind him.
Richard came to The Stone Clinic for a different answer. His goal was not simply to walk without pain. He wanted to keep running at the highest level. Here's the story of his run across the USA on two robotic partial knee replacements.


