Alternatives to Artificial Knee Replacement Reviewed
Hear From Our Patients
25-Year-Old's Disaster Knee Saved by BioKnee Program
Here is a short review of the most common alternatives to knee replacement surgery.

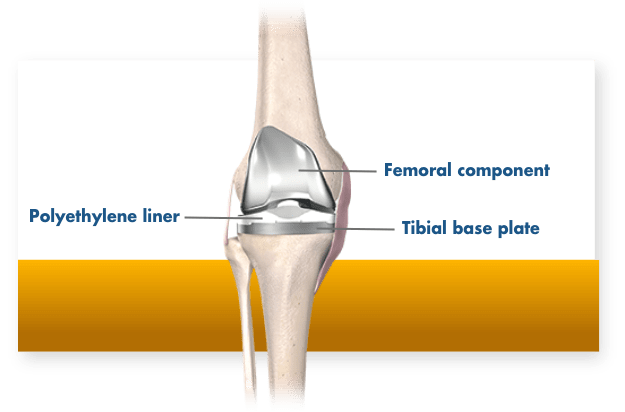
Artificial knee replacement surgery involves resurfacing the femur (thighbone) with a cobalt chrome metal cap and the tibia (shinbone) with a titanium tray, on top of which sits a replaceable polyethylene insert. Sometimes a button of polyethylene is also placed on the patella (kneecap).
While this procedure works well for people with severe arthritis involving most of the knee joint, about 80% of people told they need a total knee replacement actually don’t. They could instead have one of the nonoperative treatments listed below, a biologic knee replacement where the meniscus and articular cartilage are replaced or regrown, or a partial knee replacement where only one part of the knee is resurfaced with metal and plastic. Here are some of the most popular alternatives:
Bracing
The pros and cons of wearing a brace for an arthritic knee are many. On the positive side, a brace can limit motion, apply pressure to one side of the knee in order to unload the pain side, or just provide warmth from compression. The cons are that braces are awkward to use, the benefits don’t last very long, and stiffness often occurs. Most patients abandon them after a short while, except while playing sports.
Bottom line: Bracing can offer temporary comfort by supporting the joint, but is awkward and offers no permanent solution.
Walking Aids
Crutches, canes, and mobility devices unload joints. When forces like bearing weight are decreased, the joint surfaces become a little less stressed and often less painful. The cons are that these “aids” often limit activity, are clumsy to carry around, and really don’t solve the underlying problems.
Bottom line: Walking aids can offer relief by offloading the joint, but negatively impact gait patterns.
Physical Therapy
Arthritis leads to joint stiffness and loss of motion. The less range of motion in the joint, the more wear occurs on a smaller area of the joint, leading to faster degradation. Physical therapy, when focusing on manual hands-on therapy, is incredibly helpful for many arthritic patients. It mobilizes the tissues, increases the range of motion more than you can do on your own, and optimizes a strengthening program. The cons are the cost and the hassle factor in getting to a therapist’s office. Online or virtual therapy can be helpful, but it is nowhere near as good as a great manual therapist.
Bottom line: Physical therapy can offer significant pain relief and improved functionality. While it cannot heal damaged anatomy, it can increase strength and performance to slow the progression of symptoms.
Cortisone Injections
Corticosteroids shut down cell metabolism, therefore decreasing the fluid produced inside joints and the pain associated with it. The problem is that steroids also weaken tissues (less cell metabolism equals less collagen production) and lead to higher rates of infection.
Bottom line: Cortisone still has a role in medical care. However, far less destructive alternatives exist that can offer joint pain relief without the associated drawbacks of corticosteroids. We very rarely use cortisone anymore.
PRP (Platelet-Rich Plasma) Injections
PRP is a concentrate of the platelets from the bloodstream. Platelets contain granules loaded with growth factors that reduce joint swelling, stimulate cellular activity, are anti-scarring, anti-inflammatory, and antibiotic and immune-modulating. They also recruit the body’s own reservoir of stem cells to the site of injury. Other than cost, there appears to be no downside. When combined with a lubricating fluid such as hyaluronic acid, pain relief can be extended to 18 months in many instances. The one problem is that it doesn’t work for everybody and eventually becomes less effective at reducing the pain of arthritis.
Bottom line: PRP injections have become an important tool for orthopaedists. While there is more to learn to unlock their full therapeutic potential, the side effects are virtually non-existent, meaning that there is minimal risk in attempting to use this to relieve symptoms. PRP cannot definitively repair damaged anatomy, but can relieve painful symptoms and often help delay or avoid surgery, as well as recover faster from almost every surgical procedure.
Stem Cells
Stem cells are perivascular cells that live on the walls of blood vessels. Everyone has billions of them, though more when you are younger. When an injury occurs, a siren call to the stem cells goes out, the cells divide, and a daughter cell, often called a progenitor cell, rushes to the site of injury to direct the healing response. Individual stem cells injected directly into the joint are not as effective as they often die quickly or are not specific to the type of injury. The most effective technique is to inject factors that mobilize the most native cells. Our research foundation at www.stoneresearch.org is working on optimizing these recruitment factors.
Shockwave Therapy
Ultrasound and magnetic fields function by stimulating tissues. Shock wave therapy appears to be the most energetic of the applications and may work by creating a new injury with acoustic waves. Energy potentiates the effects of PRP and growth factor injection in part by producing micro injury to the collagen of the already injured tissues. This fresh impact sends signals that recruit the body’s reparative cells and may assist in converting inflammatory cells to proliferative reparative cells. We use it with every injection to speed the healing of bone and tissue injuries.
Arthroscopic Surgery/Debridement
All arthroscopic surgery is not the same. The cleaning out of torn tissues, loose bodies, and bone spurs from an arthritic knee has been incredibly helpful for many of our patients, specifically when the tissues are causing mechanical problems such as catching, locking, limiting motion, and swelling in the joint. Unfortunately, studies that focus on just one part of the arthroscopic procedure often fail to show definitive relief. Insurance companies often use this generic study data to limit reimbursement. But that view is not held by many top surgeons, who choose which patients can benefit and which steps to take in the surgery. Arthroscopic surgery, in which tissues are regrown or replaced, is very different from just debridement alone.
Bottom line: Debridement cannot heal arthritic knees, but can remove debris in the joint that may be the source of your pain. Many tissues are repairable in expert hands.
Osteotomy
Changing the alignment of the bones in an effort to optimize the mechanical forces in the joint can help delay the progression of arthritis and improve the symptoms. Unfortunately, osteotomy does not directly address the primary cause of pain, which most often is loss of the articular and or the meniscus cartilage. The complication rates from osteotomies are high, the good outcomes are measured in years and not decades, and the damage to future artificial joint replacement results is real. Few patients return to high-level sports after osteotomies.
Bottom line: While osteotomies may still help some patients with complex cases, we believe that it is better to solve the actual problem of tissue damage and loss rather than just change the biomechanical loading.
Microfracture
Though this procedure has demonstrated benefits for athletes in the short term, the results have generally not lasted. In its place, we perform an articular cartilage paste graft procedure. Paste grafting has been highly effective in salvaging failed microfractures and procedures such as MACI and OATS for isolated cartilage lesions. Only paste grafting has been reported to work well in both isolated chondral lesions and arthritic knees in long-term outcome studies.
Bottom line: The data demonstrates that microfracture procedures don’t last. While they can offer a short-term reprieve and return to sports, the articular cartilage paste grafting (regenerating) procedure (ArtCart) has shown long-lasting results.
Biologic Knee Replacement (BioKnee®)
In the hands of surgeons with expertise in replacing meniscus cartilage, regrowing damaged articular cartilage, and restoring ligaments in arthritic knees, the results of biologic knee replacement for arthritic knees have been gratifying, with long-term delays in coming to total joint replacement surgery. The Stone Research Foundation published our data on 85 patients over 50 years old, referred for partial or total knee replacements, who chose a biologic replacement. Over 40% of patients delayed their need for an artificial replacement for 8.5 years, and the other patients never came to a partial or total knee replacement in the course of a 2-25 year outcome study1. The cons of this approach are cost, longer rehabilitation times, and possible reinjury of the biologic tissues.
Bottom line: Biologic knee replacement extends the life of knee joints. Repairing, regenerating, or replacing natural tissues can help you delay or completely avoid artificial knee replacement. It can provide a much-needed solution to patients too young to qualify for artificial knee replacement. The possible challenge with this approach is a longer rehab time and the availability of these procedures is limited to a handful of surgeons.
Partial Knee Replacement
The introduction of robots to surgery two decades ago dramatically improved the precision with which metal and plastic implants can be placed into the knee joint (and now the shoulder, hip, and spine). This permitted a wider group of surgeons to develop partial knee replacement expertise, and for total knee replacement surgeons to more frequently abandon the use of bone cement. (The precise robotic cuts allow porous implants to be placed perfectly against the bones, allowing the bone to grow into the implant.) Partial replacement results in a faster recovery, a return to full sports, and preserves the option for resurfacing the rest of the joint at a later date if necessary. Partial knee replacements feel much more natural to patients than full replacements. We are biased to performing a partial knee over a total knee whenever possible.
Bottom line: Don’t replace what’s not damaged. A partial is better than a total, and when performed with robotics, you are much more likely to forget you ever underwent surgery. Additionally, a partial replacement can be expanded into a bicompartmental partial knee replacement or a total knee replacement later in life (if necessary). So, no options are lost.
The range of options for patients continues to expand. The goals of treatment include pain relief, range of motion improvement, and return to active lifestyles. Our general guideline is that if there is still joint space visible on X-rays, alternatives to metal and plastic are viable. Once the joint collapses to bone-on-bone, the success rates of the non-operative options and biologic replacement options decline. That said, I have many patients with horrible-looking X-rays with no joint space who come in every Fall and say “Doc, I am not letting you operate on my knee until those cocktail injections you give me stop working…They get me through the ski season, and that’s all I need.”
Article originally published July 24, 2025. Updated & republished June 21, 2026 by Kevin R. Stone, MD, with scientific and content updates.
Citation
- Stone, K. R., Walgenbach, A. W., Slatter, S., Turek, T. J., Ferguson-Dryden, C., Dicker, M., Miltenberger, E., Cowles, H., Liu, V., Wu, S., & Vessal, M. (2024). Meniscus allograft transplantation in conjunction with arthroscopic biologic knee restoration delays arthroplasty in patients older than 50 years. Arthroscopy. Advanced online publication. https://www.sciencedirect.com/science/article/pii/S0749806324004183?dgcid=author

