How Do You Know If Your ACL Surgery Failed?
Hear From Our Patients
ACL Surgery Revision Reconstruction Patient 6 Years Post-op
ACL surgery is performed more than 100,000 times each year in the U.S., by a variety of different techniques. How do you know if your surgery worked?

First, let’s look at what gets you there to begin with.
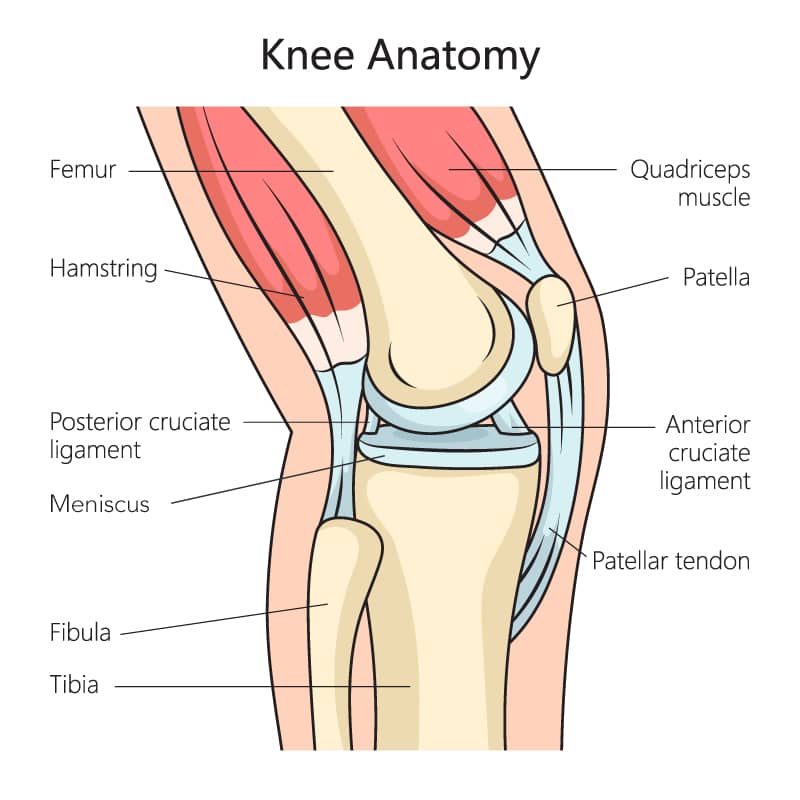
“Doc, I pivoted, and my knee gave way.” Or “Doc, I hyperextended my knee and heard a pop.” Those, and a host of other stories, reveal a torn anterior cruciate ligament. To protect the knee, avoid tearing the meniscus cartilage, and return to sports with a stable knee, most athletes request ACL surgery. This usually means replacing the ruptured ligament with either a tendon from the quadriceps, hamstring, or patella, or a donor tendon. Surgery is followed by a year-long rehabilitation program designed to improve the range of motion and strength of the muscles of the lower extremity—and of the entire athlete.
When returning to sports, the knee is either stable or it isn’t. It can flex through a full range of motion, or it can’t. It swells and hurts, or it doesn’t. Successful ACL surgery means that the femur rolls back and rotates on the top of the tibia in a normal fashion, maintaining stability at every point in the arc of motion. This allows the patient to return to full pivoting sports without a loss of function.
If the ACL ligament is replaced in a non-anatomical direction—most commonly with the femoral hole too high in the intercondylar notch, or too far forward on the femur, or the tibial hole too centrally placed on the top of the tibia —the knee will be stable at 30 degrees of flexion but unstable at 90 degrees. The ligament reconstruction thus fails to protect the knee, meniscus tears happen more often, and arthritis sets in.
When ACLs rupture, not just the ACL is injured. The corners of the knee are often stretched, and the meniscus cartilages torn.
If the surgeon fails to recognize the rotational instability from those corner cartilage tears, the knee will be stable during forward and backwards motion but unstable with rotational stress. The MRI often misses this part of the injury. It is so common that now most ACL surgeons add an additional procedure called a lateral extra articular procedure (LEAP) to their ACL surgery. This reduces the reported failure percentage rate from the mid-teens (or higher) to single digits. LEAP may also be called ALL (or anterior lateral ligament), or other names for procedures that reinforce the lateral side of the knee.
Meniscus tears in hard-to-see places—such as the skirt ligaments at the back of the meniscus—are also common with ACL injuries. Failure to repair them leads to a high rate of both ACL failure and further meniscus tearing, which causes pain, swelling, and catching in the knee. The reason that 50% of ACL-injured patients develop knee joint arthritis after 10 years may be due to these two often unrecognized injuries.
ACL injuries are an opportunity for the athlete to focus on a full-body fitness program and should permit people to return to sports better than they were before they were injured. The rate of recovery is slow, often taking up to a year to return to sports. How to accelerate this healing is a subject being researched by our clinic and others. The more frequent addition of growth factors, lubrication, and progenitor cells may be helpful. Testosterone therapy, at the time of surgery and in the immediate postoperative period, is another focus of our research on accelerating healing. In any case, you know your ACL surgery (or its rehab) has failed if you are unable to push yourself and your knee as hard as you wish, with only your drive holding you back. Our goal is to make it a forgotten knee.
ACL Revision Surgery - The Keys To Getting it Right
If a patient's first ACL surgery is unsuccessful, a revision surgery is necessary. The original surgery usually fails due to other knee issues beyond just the ACL. Identifying and correcting all issues within the knee is critical in achieving a positive, long-term outcome. That’s why, at The Stone Clinic, we look carefully at everything going on inside the knee—not just the ACL—to fix all the issues that could affect recovery. Our goal is to give the new graft the chance to heal well, allowing our patients to return to their favorite activities, Fitter, Faster & Stronger than they were before their first surgery.