Who Needs an ACL?
Hear From Our Patients
ACL Revision Reconstruction Surgery Patient
Anterior Cruciate Ligament (ACL) injuries happen hundreds of thousands of times annually in the U.S. alone. Repairs and reconstruction occur about 400,000 times per year. Who gets and who needs an ACL?
The answer is, not everyone.
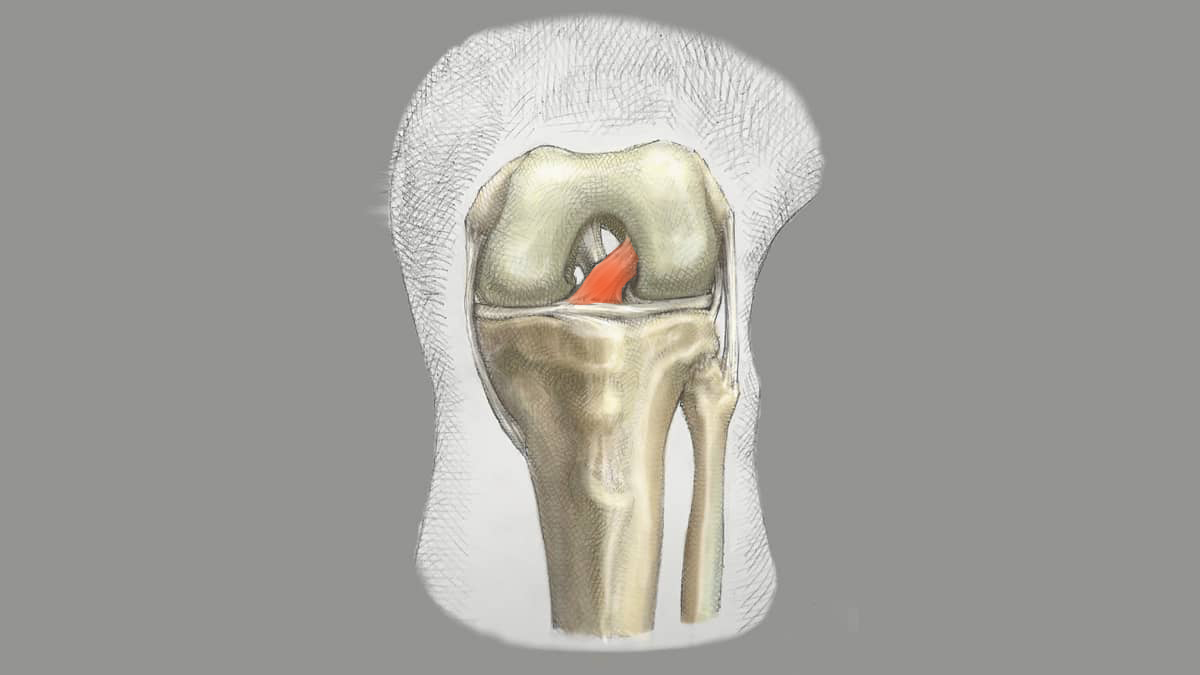
The ACL is the key guidewire for the knee joint. Stretching from the femur to the tibia, the ligament is often injured in twisting sports such as soccer, basketball, skiing, football, and rugby. Though primary suture repair of some ACL injuries is possible, replacement of the torn ligament (called ACL reconstruction) is the most common surgical treatment.
Most athletes with ACL reconstruction lose up to a year of activity before they can return to their previous level of sports performance, and only two-thirds of athletes ever do return fully. There is a reinjury or failure rate of up to 15% for many reconstruction techniques, whether the patients’ own tissues or donor tissues are used. New techniques—such as adding additional tissue support to the ACL repairs and certain reconstructions (e.g., lateral extraarticular procedures)—have been shown to reduce the failure rate to single digits. But complications such as stiffness, scar tissue, loss of motion, and infection can markedly lower the success rates.
Certain knees are ACL dependent, and others are ACL independent, meaning they function perfectly well without an ACL. Certain athletes don’t notice the instability, and certain sports don’t seem to rely on the ACL for stability. How do you determine where you fit?
You can’t. You are used to your knee as it is. Once injured, you don’t know for sure how unstable you will be. An experienced doctor can usually make this determination. The first step is a careful physical exam. Knees that have a large amount of laxity or play on exam and a pivot shift (a clunking of the tibia as it reduces on the femur in a physical exam) are most likely ACL dependent and will do poorly without one. Knees that hyperextend or have excessive rotation on exam also do poorly. People with marked joint laxity or hypertension need their ACLs. Most athletes in twisting and pivoting sports are ACL dependent, needing the ACL both to perform well and to protect the meniscus and articular cartilage within the knee joint.
Some people with a complete ACL tear, however, have only mild instability or sometimes none at all. These knees are called ACL independent. And some people with loose knees after an ACL injury, simply don’t mind the looseness and perform just fine. Other ACL tears heal naturally to the surrounding tissue, usually the PCL, providing just enough stability to avoid the request for surgery.
Many active people under the age of 50 who rupture their ACLs do undergo stabilization surgery. The surgical techniques and the outcomes vary with the bias and experience of the surgeon. The question of whether or not you need an ACL repair, who should do the surgery, and what technique and which tissues are used are all variable and cannot yet be fully controlled—not even by AI agents.