Meniscus Tears Updated
Hear From Our Patients
30-year-old Avoids Arthritis with Meniscus Replacement Program the BioKnee
The meniscus is the key fibrocartilage shock absorber in your knee. When it is torn, the knee doesn’t function properly. Here is how it works (or doesn’t):
The meniscus has a partner. One side of the structure is called the medial meniscus, on the inside part of your knee; the other is called the lateral meniscus, on the outer side of the knee joint.
These are separate structures, linked by a transverse ligament. Both are attached primarily to the tibia (shin bone) by meniscus tibial ligaments around the circumference. Both move within the knee as the knee flexes and extends, the lateral side as much as 1.5 cm. Both have circumferential collagen fibers that absorb the hoop stresses the body places on the knee, and radial tie rods to hold these fibers together. Each has unique fibrous cells called fibrochondrocytes and stem cells that help the tissue repair itself after minor injuries. There are naturally charged sugars called glycosaminoglycans that absorb and release water with every step. This complex organization has made it impossible to invent a successful artificial meniscus replacement. The invention would have to be soft enough to absorb the forces (2-3 million steps per year up to 5 times the body weight), strong enough not to tear, yet durable enough to rub against both normal cartilage and rough articular cartilage without creating wear particles in the knee. Only a living tissue has all of those properties.
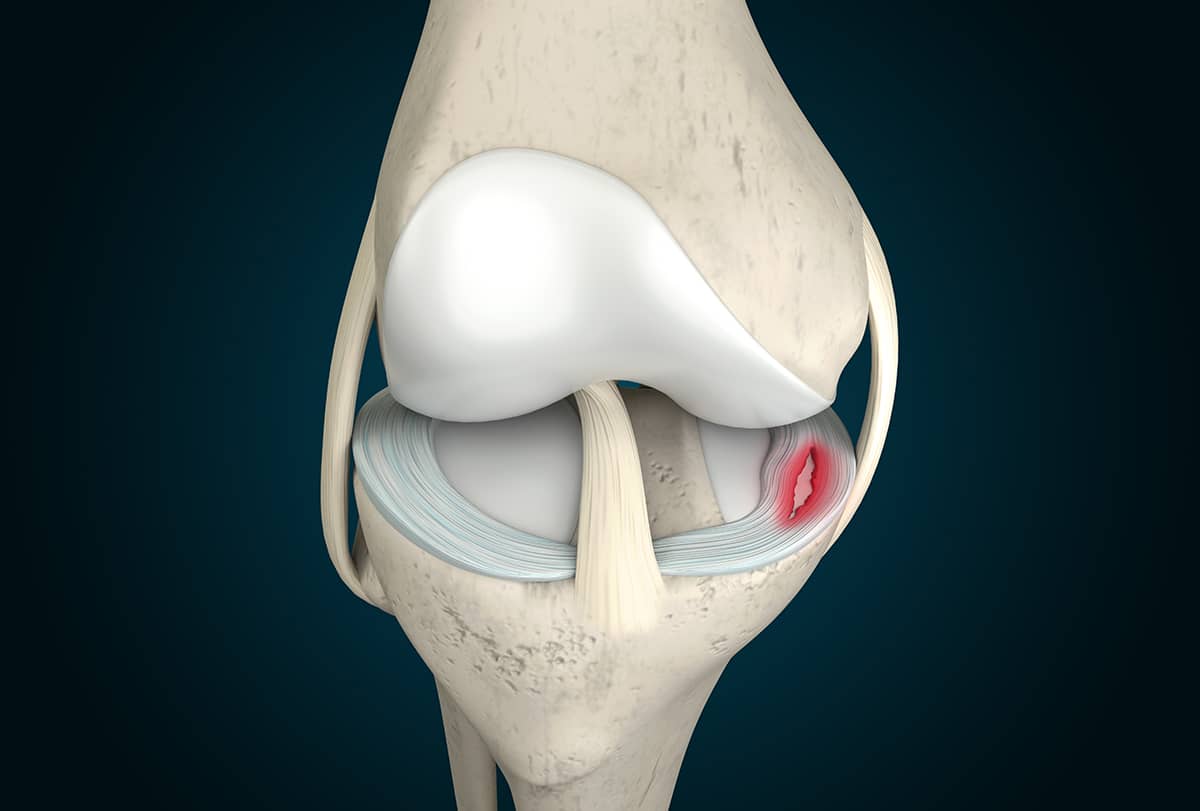
When the meniscus is torn, the concentration of forces on the top of the tibia is concentrated on a smaller area due to the disruption of the collagen fibers. With every step, the torn meniscus separates a little until, over time, it degenerates. The surfaces below the cartilage see excess wear due to the higher forces. The wear leads to arthritis, exposing the underlying bone.
Decades ago, surgeons shifted from removing the torn tissues to repairing them whenever possible. Today, orthopaedic science and techniques have improved so much that many previously thought-to-be-irreparable are now, in fact, repairable. New suture techniques and devices, along with augmentation with marrow progenitor cells and growth factors from PRP, bone marrow, and fat, have improved the success rates of meniscus repair. Unfortunately, too many repairs still fail. The most common failures are the “bucket handle” tears, where part of the meniscus was displaced into the middle of the knee joint, or the previously repaired meniscus that has retorn and the root tears, where part of the posterior horn of the meniscus rips out of the bone. Each of these failures may be in large part due to the degeneration of the meniscus tissue after tearing, resulting in a lack of healthy tissue to heal. This is one reason why the sooner after injury the meniscus is repaired, the better.
You, the patient, often feel renewed pain when bending the knee, pivoting in sports, or just getting out of a car. Catching or locking the knee is highly associated with a meniscus tear, as is swelling behind the knee called a Baker’s cyst. In fact, Baker’s cysts are associated with a posterior meniscus tear 85% of the time. Unless the meniscus is repaired, the cyst continues to form.
MRI is great for diagnosing a meniscus tear, but not so great for determining if a repaired meniscus is healed. This is because a repaired meniscus often shows a white fluid signal at the repair site for years after the repair. This makes it confusing to determine if we are looking at the healed but scarred meniscus tissue or a true re-tear. The patient’s symptoms are the best guide.
Repairing meniscus tears in young people (under age 50!) is critical, as most people under 50 have decades to go of loading their knee joints. After age 50, there is some debate, as the collagen tissue can be more brittle. However, my patients, those who want to die at age 100 playing the sports they love, need a healthy meniscus just as much as a younger person. Therefore, we push the techniques to repair and add biologic augmentation to as many of these as possible. If too much meniscus is degraded or lost from a previous surgery, we replace it with a donor (allograft) meniscus.
Even arthritic knees benefit. We published data on patients over fifty who were referred to us for an artificial partial or total knee replacement. These patients instead underwent an articular cartilage repair with a paste graft technique and a meniscus allograft. Our 2-25 year outcome study showed that 42% of these patients obtained, on average, an eight-year delay before needing an artificial joint. For 48%, no artificial joint replacement at all has been necessary. We continue to follow these patients.
The best advice is to repair the torn tissue as soon as possible and replace it if too much is missing.
Meniscectomy vs Meniscus Replacement
When the meniscus tears, the treatment choice matters. A meniscectomy removes the torn portion of the meniscus. A meniscus repair uses sutures to preserve and heal the tissue. A meniscus replacement, also called a meniscus transplant or meniscus allograft, replaces missing meniscus tissue with donor cartilage.
At The Stone Clinic, our bias is clear: repair the meniscus whenever possible and replace it when it is irreparably damaged or missing. The earlier the knee's shock absorber is restored, the better the chance of protecting your joints for a lifetime.