ITB Tendonitis
The iliotibial band running (ITB) from the hip down the outside of the leg is often a source of pain for athletes of all activities. Here are a few of the troubles, and the solutions.
The iliotibial band is named for its origin and point of insertion. The ilium is part of the hip bone, while the tibia is the large bone of the lower leg. The name is not entirely accurate, as the band also has insertions on the patella (kneecap), which causes all kinds of problems for some people.
Starting at the hip joint, the most common complaint is pain at the outside of the hip. People come into our clinic worried that they have hip arthritis. Most of the time, however, the pain is due to an inflamed bursa: a layer of tissue just underneath the thick collagen fibers of the iliotibial band. This bursa (called the greater trochanteric bursa) becomes enlarged when the ITB rubs over the bump of the femur (the trochanter) in just the wrong way, irritating it. The inflammation causes pain, and the person sometimes walks with a slight limp, worrying that their sports days are limited. Fortunately, the bursa is not in the joint, so anti-inflammatory injections and drugs can be used safely in this location. Soft tissue massage and physical therapy to improve gait and muscle strength are usually curative in a few weeks’ time.
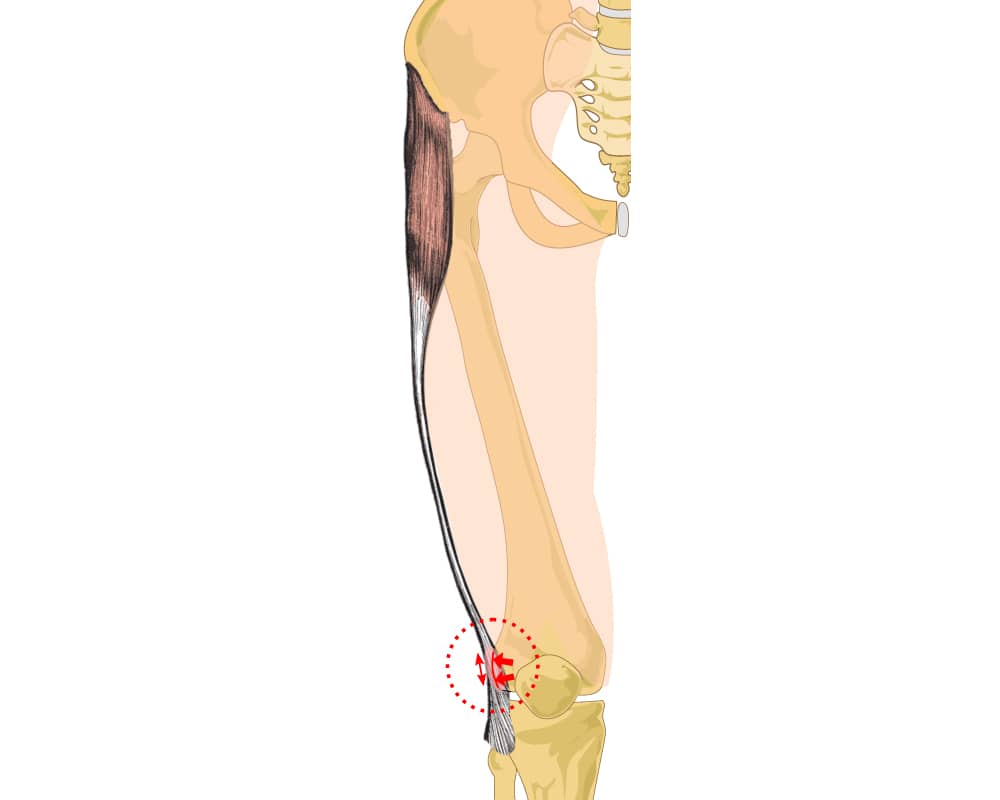
The ITB courses down the outside of the leg, sending firm fibers to the kneecap and to the bump on the outside of the tibia, called Gordy’s tubercle. When the band is tight, a friction syndrome can occur due to rubbing on the underlying tissues. Bicyclists, cross country skiers, and rowers complain of pain on the outside of the leg at the knee joint. Stretching the ITB with foam rollers, and massage, are often helpful. For cyclists, adjusting the seat height—which changes the angle of the knee during pedaling—can sometimes eliminate the problem.
When the kneecap is tilted over to the outside of the knee, as is often the case for people with tight tilted kneecaps, the fibers of the iliotibial band may be to blame. Mobilizing the kneecap with a high-tech device commonly known as a small toilet plunger is an incredibly effective way of loosening the kneecap and solving the problem. Great physical therapy with manual soft tissue mobilization, combined with muscle strengthening, can guide the kneecap back to a more central position.
If injections, anti-inflammatories, stretching, massage, and activity modification fail, a surgical lengthening of the ITB can do the trick. In the past, surgeons would often release the fibers to the kneecap—a procedure called a lateral release. But as these fibers are critical for guiding the kneecap motion, this led to substantial complications for many patients. Lengthening of the ITB alone can now be done safely and effectively through a very small incision.
The iliotibial band plays an important role in stabilizing both the hip and the knee. When painful, it is telling us that the motions of this structure—and sometimes the entire body—are not symmetrical and require re-balancing. Just because the ITB is on the outside of the leg doesn’t mean it isn’t an important internal structure.
