Achilles Tendon Pain
Hear From Our Patients
Double Achilles Injury Patient Compares Percutaneous Repair to Open Surgery
The Achilles tendon often becomes painful for athletes of all ages. Here is the update on the problem and the cures.
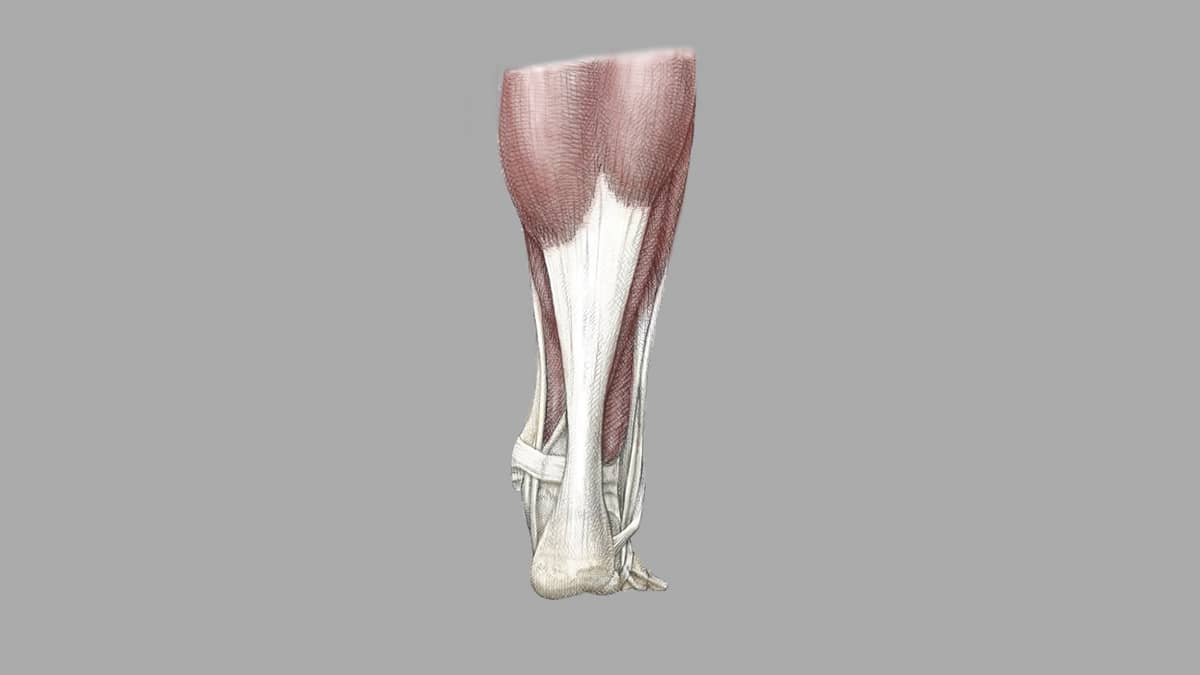
Original illustrated artwork by: Katerina Salsman
The Achilles is a broad, thick tendon that passes within a thin sheath. It stretches from the muscles in the calf (gastrocnemius and soleus) to the bone of the heel (calcaneus). The tendon is designed to stretch as we walk, permitting a powerful push-off of the foot. Sometimes, however—when landing from a jump or simply walking in badly fitting shoes—we irritate or tear the tendon in such a way that it does not heal. Pain and often swelling result.
The Achilles tendon is composed of a mixture of interwoven collagen fibers. These fibers have chemical crosslinks that, depending on your genetic makeup, can either make for a very flexible tendon or one that is quite stiff. In general, it is the stiff ones that get irritated and torn.
You can think of all tendon injuries in these simple terms: stretch injury, mild tear, moderate tear, or complete tear.
In a stretch injury, the collagen fibers are pulled but not torn. The elongation of the fibers stimulates a mild healing response. This includes a release of fluid from the local cells and a localized inflammation process. A small amount of blood and its reparative cells rush to the site of the stretched fibers. Normal healing occurs without a scar as the fibers themselves have not been torn.
The second and third levels of injury—mild to moderate tearing—involve a more robust healing response. Bleeding occurs from the torn blood vessels within the tendon and, sometimes, from the sheath itself. Swelling and pain accompany the tearing. The signals sent to the brain call for splinting the injury and limiting motion. This natural internal immune response floods the torn tissues with macrophage blood cells: one type to clean up the torn fibers and another to induce the production of new collagen by the local cells. This process is augmented as the body releases stem-cell-derived self-repair cells from the perivascular to the torn collagen fibers. A new body of research also suggests that the collagen itself can respond to the injury independent of the native cells, providing a self-assembly process for certain types of injury.
Most of the time this remarkable process induces the torn tendons to heal—often with slightly thicker fibers and if exercise is applied occasionally, with a stronger tendon.
The fourth type of injury—the complete rupture of the Achilles tendon—can heal on its own. Usually, however, due to the pulling of the calf muscles and separation of the torn ends of the tissue, the gap is filled with disorganized scar tissue. The tendon ends up in an elongated position, leading to weakness of foot push-off. For this reason, most surgeons caring for injured athletes will repair the tendon with sutures to restore its optimal length. In our hands, these repairs are done percutaneously. We suture through tiny punctures in the skin, preserving the tendon sheath and the natural healing blood clot that forms around the torn fibers.
Unfortunately, it is possible that, with any of these injuries, the otherwise elegant healing process within the tendon fails to complete its job. This leads to tendinosis (formerly called tendonitis or tendinitis), an area of collagen tissue degeneration. The ends of the torn fibers die and, in the degradation, release catalytic enzymes that further break down the surrounding tissue. This tendinosis is not an inflammatory problem—which is one of the reasons why injections of cortisone, which inhibits cell metabolism when shutting down inflammation, only make the process worse.
Tendinosis will sometimes respond to mechanical stimulation from soft tissue massage, electrical and magnetic current, heat and ultrasound, shockwave therapy, and other forms of stimulation. The reason for the response is that the cells have mechanoreceptors on their surfaces. When energy is applied these receptors are stimulated, telling the cell to produce more collagen.
Injections of growth factors and cytokines to induce stem cell responses can work, but only if the degeneration is neither too severe nor surrounded by chronic scarring.
Surgical intervention—with excision of the degenerated area, repair of the tissues, and stimulation of a new blood supply—usually cures the problem. After surgery, we apply growth factors and cytokines to direct robust healing and avoid the degeneration cycle mentioned above.
So if you injure your tendon, pay attention. Grade the injury and apply the latest therapies to the damaged tissue. Almost all repairs do better with gentle graded stretching and strengthening, as long as these activities stay within a range of motion that does not further injure the tissue. Never let the injury persist for months on end, as tendons should mostly heal within the first few weeks. Don’t let your Achilles tendon become your Achilles heel.