Knee replacement: Partial can be just as good as total
A man came in to see me recently convinced he needed a total knee replacement. He’d spent most of his life outdoors and most winters skiing but now he was in horrible pain, and it seemed like those days on the slopes were over.
He told me that he couldn’t climb stairs and said that he found it difficult to walk distances. He explained that, over the years, he had various operations to clear out problems with his knee but he had been told he had reached the end of the road for these small operations and it was time for the “big one.”
A total knee replacement means swapping the worn-out, painful knee joint surfaces with metal and plastic components. It involves placing a metal end on the thighbone (the femur) and a metal and plastic tray on the shinbone (the tibia). However, knees do not necessarily wear out evenly, sometimes one part of the knee is perfectly fine while another part is completely destroyed. If only part of the knee joint is worn out, why replace all of it?
I’ve dedicated much of my career to developing new ways to preserve the natural biology of the knee, to offer an alternative to artificial joint replacement. My bias is toward BioKnee solutions, which can rebuild and regenerate joints using donor tissue and native repair cells. Sometimes the damage is too much for a BioKnee, but it still does not warrant a total knee replacement. Just as for a cavity in your tooth, you would want a filling, not a set of dentures. For a partially worn out knee, you would want a partial knee replacement, not a total replacement.
MRIs and X-rays revealed that the man who had come to see me was beyond a BioKnee but didn’t, after all, need to have the “big one.” Instead, I explained that I’d be performing a partial knee replacement, assisted in surgery by a robot.
A partial, or unicondylar, joint replacement involves resurfacing the worn-out portion of the joint, either the inside, outside, or kneecap, and leaving the rest of the joint alone. To work properly, the components must be put in extremely accurately. Even a millimeter or two of tilt or rotation dramatically affects the wear patterns and longevity of the components. Think of how a car out of alignment means rapid tire wear.
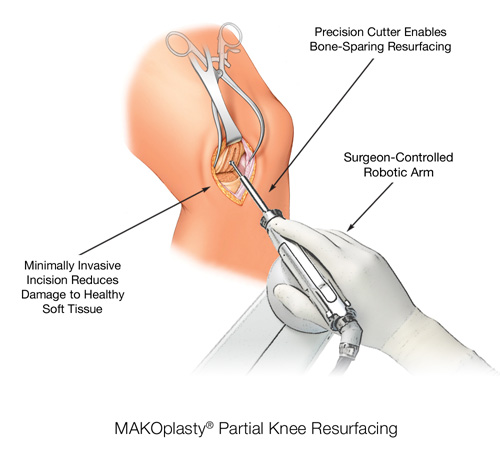 With my robotic assistant, I can plan the surgery on a computer screen with a virtual model of the patient’s own knee (built-in 3-D from their CT scans). I can put the components in place virtually and adjust them before making only a small incision.
With my robotic assistant, I can plan the surgery on a computer screen with a virtual model of the patient’s own knee (built-in 3-D from their CT scans). I can put the components in place virtually and adjust them before making only a small incision.
During surgery, the robotic arm and computer navigation provides me with pinpoint precision to enable optimal implant positioning and alignment that results in a more natural knee motion.
Afterward, people tell me that their knees feel normal, which almost never occurs after a full knee replacement.
With a partial knee replacement, there is no need for saws, drills or guides. In fact, the procedure is so minimal that you can walk out of the surgery center 1½ hours after surgery and begin physical therapy the next day.
Far from having to give up skiing for good, as my patient had feared, I explain to him that I won’t restrict him in any way after surgery and that all being well, he’ll be back skiing again this season, no problem.
Hear from patients who have had a partial knee replacement.
Arthritis of the knee is when you've lost the soft cushioning at the end of your joints and your bones are rubbing together. If the arthritis is too severe for The Stone Clinic's bioknee procedure but not bad enough for you to need the whole joint replaced, a partial knee replacement is possible.
